Research Programme: Liver Transplant for Hepatocellular Carcinoma
Principal Investigator: Prof. Giuseppe Tisone

Prognostic Outcomes in liver transplant (LT) for hepatocellular carcinoma (HCC) continues to challenge the field. Although Milan Criteria (MC) generalized the practice of LT for HCC and improved outcomes, its predictive character has degraded with increasing candidate and oncological heterogeneity.
The Tor Vergata group, headed by Prof Tisone, in collaboration with other Italian, European, Asian and North American liver transplant centres, sought to validate and recalibrate a previously developed, preoperatively calculated, continuous risk score, the Hazard Associated with Liver Transplantation for Hepatocellular Carcinoma (HALTHCC), in an international cohort.
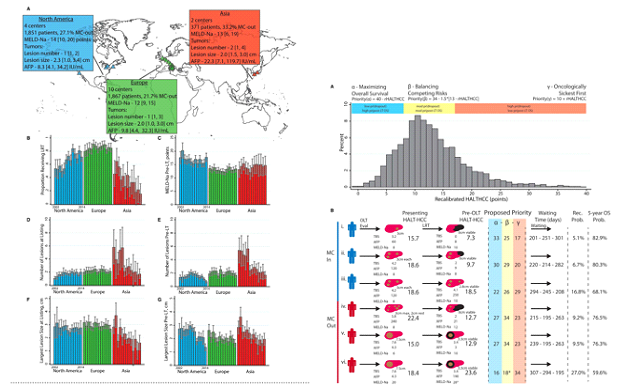
From 2002 to 2014, 4,089 patients (both MC in and out [25.2%]) across 16 centres were included. A continuous risk score using pre‐LT levels of alpha‐fetoprotein, Model for End‐Stage Liver Disease Sodium score, and tumor burden score was recalibrated among a randomly selected cohort (n = 1,021) and validated in the remainder (n = 3,068).
This study demonstrated significant heterogeneity by site and year, reflecting practice trends over the last decade. On explant pathology, both vascular invasion (VI) and poorly differentiated component (PDC) increased with increasing HALTHCC score. The lowest‐risk patients (HALTHCC 0‐5) had lower rates of VI and PDC than the highest‐risk patients (HALTHCC > 35) (VI, 7.7%[ 1.2‐14.2] vs. 70.6% [48.3‐92.9] and PDC:4.6% [0.1%‐9.8%] vs. 47.1% [22.6‐71.5]; P < 0.0001 for both). This trend was robust to MC status. This international study was used to adjust the coefficients in the HALTHCC score. Before recalibration, HALTHCC had the greatest discriminatory ability for overall survival (OS; C‐index = 0.61) compared to all previously reported scores. Following recalibration, the prognostic utility increased for both recurrence (C‐index = 0.71) and OS (C‐index = 0.63).
Clinical Perspective: This large international trial validated and refined the role for the continuous risk metric, HALTHCC, in establishing pre‐LT risk among candidates with HCC worldwide. Prospective trials introducing HALTHCC into clinical practice are warranted.